Lactation Interrupted: Impact of PFAS on Breastfeeding
New commentary highlights the need to stop ignoring the potential for PFAS to disrupt breastfeeding.

As much as PFAS have been in the news of late, PFAS-impacted communities may not be aware of the impact their exposure may have had on their ability to breastfeed. Our new commentary highlights the need and opportunity for the scientific and medical communities and regulatory bodies—who have historically dismissed and downplayed the importance of this health end point—to protect this important aspect of women and children’s health. In doing so, we also hope to raise awareness of the link between PFAS exposure and difficulties in breastfeeding so that impacted mothers can seek additional support if needed.
Good for the baby, good for the mom
There are many benefits to mothers and infants from breastfeeding, so much so that medical experts such as the American Academy of Pediatrics and World Health Organization have increased their recommended duration of breastfeeding to two years. Lifelong health benefits of breastfeeding include optimized nutrition and immunological protection for infants and the reduced risk of developing certain chronic diseases such as breast and ovarian cancers, type 2 diabetes, and hypertension for mothers. Given the importance of breastfeeding on a mother and child’s health, one would expect anything interfering with a mother’s ability to breastfeed to be highly scrutinized and resources to be expended to address the problem. Yet, the negative impact that environmental chemicals can have on the ability to breastfeed is mostly ignored, including recently by the nation’s experts on breastfeeding.
Environmental impacts: The missing puzzle piece
In the United States, breastfeeding is often viewed as a choice, and a large body of research has focused on factors related to breastfeeding motivation and social support needs. But what if the physical act of breastfeeding itself has become harder?
Successful lactation depends on infant demand as well as normal mammary tissue development during puberty and pregnancy. Breast development and breastfeeding is regulated by complex hormonal processes and is vulnerable to disruption by environmental chemicals. Toxic chemicals in our drinking water and products in our homes have been associated with many health impacts, and the ability to breastfeed is no exception.
Years of public campaigns have resulted in record-high initiation of breastfeeding, with approximately 84 percent of mothers initiating breastfeeding. Yet despite the motivation to breastfeed, fewer than 40 percent of infants receive breast milk at one year of age, well below the national goal of 54 percent. Clearly, motivation and social support of breastfeeding is important—but they may not be sufficient to reach breastfeeding goals. A large, very important piece of the puzzle is missing.
Despite many women reporting difficulty in starting and continuing breastfeeding and the increasing awareness of the impacts of toxic chemicals on public health, the role of environmental chemicals has been given little attention in the breastfeeding literature and in the medical community. Most notably, the National Academies of Sciences, Engineering, and Medicine (NASEM) report on breastfeeding in the United States does not address the potential impact of any environmental chemicals. Government agencies that regulate environmental chemicals have often overlooked the impacts of chemicals on breast development and a woman’s ability to breastfeed as well.
PFAS as a case in point
PFAS (per- and polyfluoroalkyl substances) are a class of thousands of man-made chemicals that are widely used in consumer and industrial products. Due to their extreme persistence (thus, their nickname of “forever chemicals”) and widespread use, PFAS contaminate most of our environment and even our bodies. PFAS are linked to a host of serious health harms, including cancer, developmental and reproductive harm, and interference with the proper functioning of the immune and hormone systems.
Several studies of women and babies indicate that women with higher levels of PFAS in their blood do not breastfeed as long compared to mothers with lower levels of PFAS in their blood. And studies in animals have demonstrated that exposure to PFAS severely disrupts the development of mammary glands, which are essential for nursing. Taken together, this suggests that exposure to PFAS might impact a woman’s breast tissue development and ability to breastfeed.
Yet, there is a history of ignoring or dismissing the potential impacts of PFAS exposure on a woman’s ability to breastfeed in both clinical and government decision-making. In collaboration with other experts, our new commentary outlines this history and provides recommendations for how the regulatory, research, and medical communities can begin to address this important women’s environmental health effect.
Decades of evidence of harm; failure to adequately protect health
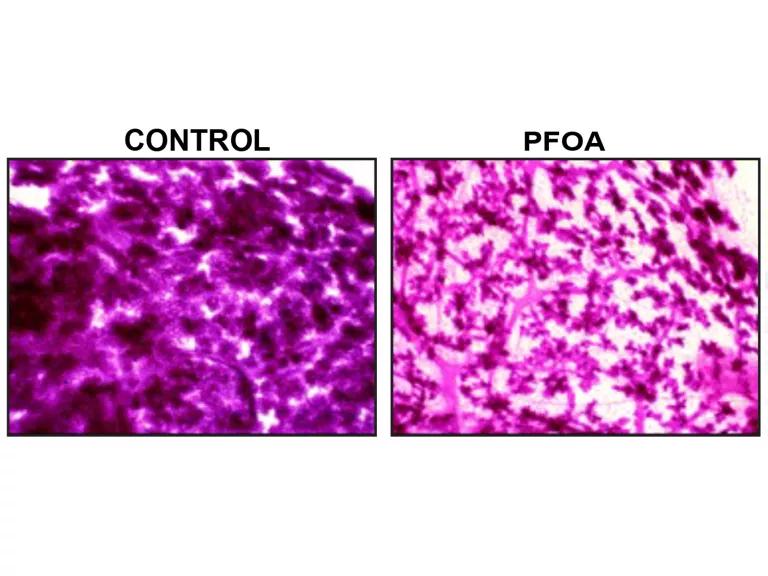
Despite a growing body of human and animal toxicological evidence, there has historically been minimal attention paid to the effects of PFAS on mammary gland development or function in risk management analysis and decisions, including in several pivotal risk assessments and policy documents. For example, the U.S. Environmental Protection Agency (EPA) has repeatedly ignored findings such as those from a 2007 study that found mice exposed to PFOA had underdeveloped and delayed mammary gland differentiation. In other words, their mammary glands were not developed and ready to nurse the litters they were about to birth.
The EPA also inappropriately interpreted a 2011 study in mice in which scientists tried to determine if lactation was impaired in PFOA-exposed mice. The authors noted that baby mice from PFOA-exposed mothers only gained one-third of the weight of baby mice from untreated mothers during a timed lactation challenge and were on average 84 seconds slower to begin suckling. The study authors noted that they did not test for other compensatory behaviors, including the total number of nursing events or the length of nursing events. However, because baby mice from the exposed mothers did not weigh less, the EPA concluded that there was no evidence of harm to lactation from the PFOA exposure. Other agencies have repeated this conclusion without re-examination.
Human studies have begun to catch up. Five of six human studies evaluated in a 2023 systematic review found shorter duration of breastfeeding is associated with higher PFAS levels, regardless of study location or study design. Similar findings were reported in two of three studies published since the 2023 systematic review. Taken together with the animal studies showing disruption of mammary gland development, the evidence strongly points to PFAS exposures harming a mother’s ability to breastfeed. Yet regulatory bodies have not integrated all available evidence nor updated their conclusions on this health effect.
This likely contributed to a missed opportunity in providing support to PFAS-impacted mothers through the NASEM Guidance on PFAS Exposure, Testing, and Clinical Follow-Up. For example, if it is known or suspected that a mother had elevated PFAS exposures, a clinician might encourage the mother to seek additional lactational support services early. Simply knowing about the potential of this health impact is also important for mothers impacted by PFAS exposure:
As a mom of two with a third on the way, I’m constantly bombarded with what I’m doing wrong and what I could be doing better. I wasn’t able to produce enough milk for my second child, and I had to supplement with formula. I know I’ll have the same struggles with my third, who will be born later this year. This has had a negative impact on not only my mental health as a mother but also on our budget since we had to purchase formula. This makes me feel like I wasn’t doing enough to nourish my child—my body wasn’t enough.
To know that something I unknowingly had been exposed to without my permission might be impacting my milk production is scary and frustrating. But it’s also helped me understand that I am doing all I can for my child. I haven’t done anything wrong. It’s out of my control. I don’t deserve to feel shame. And understanding this has given me a sense of support when I pump and helped me embrace that, despite low milk production, I’m still doing the best I can.
Avonna Stark, state director of Clean Water Action, Minnesota
What should be done?
It is time for the government agencies that are responsible for regulating environmental chemicals to stop ignoring or dismissing the harmful impacts that environmental chemicals like PFAS can have on mammary gland development and breastfeeding. Breastfeeding is important to the health of infants and mothers and anything interfering with a mother’s ability to breastfeed should be investigated, and resources should be expended to address the problem. At minimum, evidence of the disruption of mammary gland development and/or the ability to lactate should be properly acknowledged and protected against in risk assessment, and testing for effects on mammary gland development should be required before new chemicals are approved.
Outreach to health-care professionals should be conducted to increase awareness of the negative impacts that environmental chemicals can have on the ability to breastfeed. Health-care professionals should be encouraged to investigate suspected environmental exposures with their patients. Women who suspect increased exposure to chemicals that disrupt mammary gland development and function can then be encouraged to seek professional guidance and support from lactation specialists.
This paper does not address the issue of PFAS transfer from mother to baby via breast milk. However, we acknowledge that many women, especially in highly impacted communities, are eager for guidance on this topic, and we call on the scientific and medical communities to address this.
In our community, we have three year olds with kidney cancer who may never get a chance to do something as simple as ride a bike. We have mothers who are afraid to breastfeed their babies due to high levels of PFAS found in their breast milk. As a mother, I was told that my PFAS exposure might have caused my child’s cancer. No one should have to endure that kind of guilt. We need stronger regulations, so no one has to hear the words “Your child has cancer.”
Joanne Stanton and Hope Grosse, cofounders of Buxmont Coalition for Safer Water
This NRDC.org blog is available for online republication by news media outlets or nonprofits under these conditions: The writer(s) must be credited with a byline; you must note prominently that the blog was originally published by NRDC.org and link to the original; the blog cannot be edited (beyond simple things such as grammar); you can’t resell the blog in any form or grant republishing rights to other outlets; you can’t republish our material wholesale or automatically—you need to select blogs individually; you can’t republish the photos or graphics on our site without specific permission; you should drop us a note to let us know when you’ve used one of our blogs.
Related Blogs

Communities and Workers Deserve Robust Protection from Chemical Disasters

Trump EPA Proposes Toxic Loophole for Plastics Incineration
